Opioid addiction
This is a patient simulated task. The task assesses:
- Information gathering
- Communication with patient
- Applied clinical knowledge
- Patient safety
You are about to see, Mary Williams, a 25-year-old lady, in her 1st pregnancy. She is here for a booking visit at 16 weeks.Your task is to:
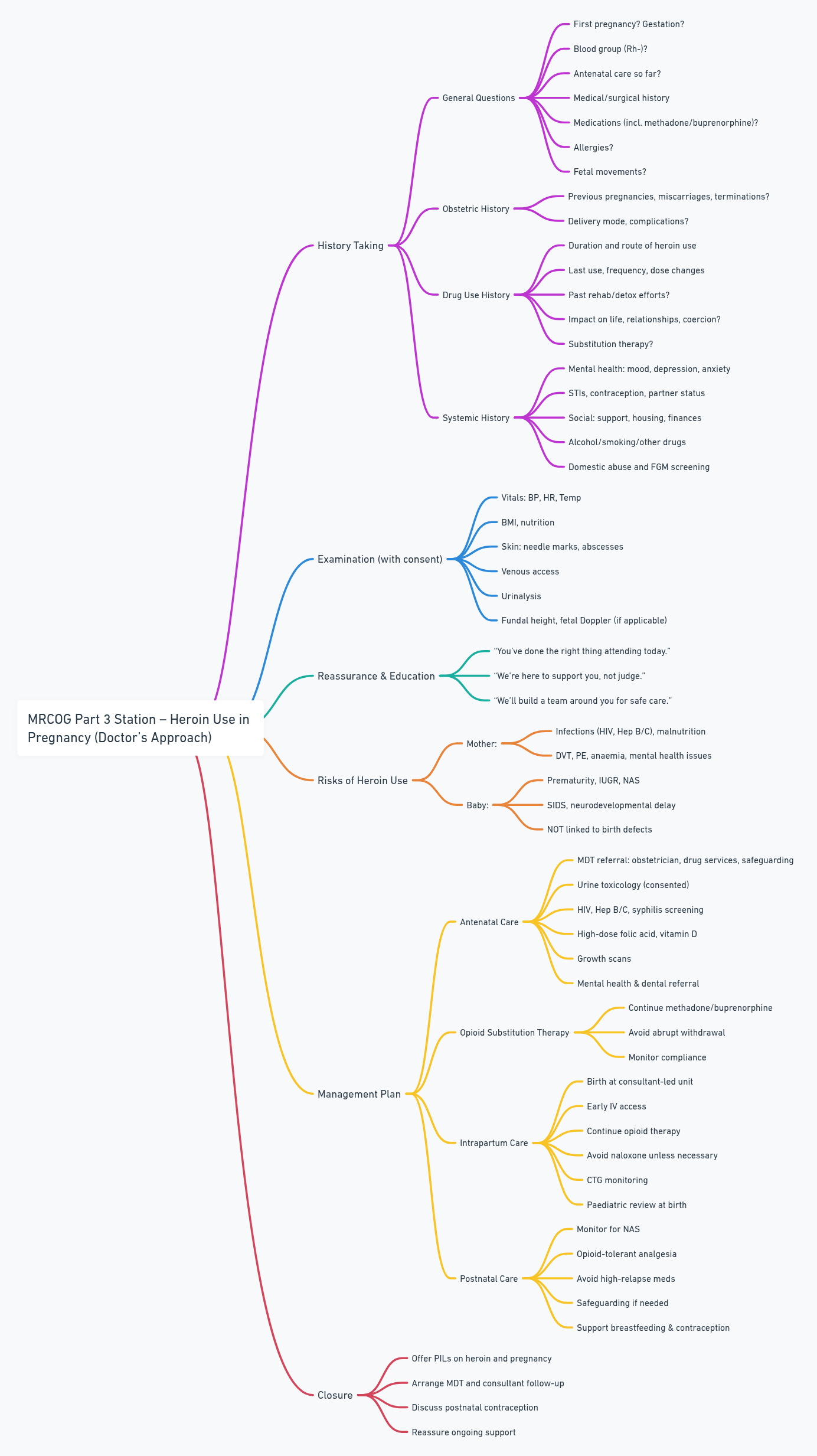
- Take relevant history
- Address her concerns
- Formulate a management plan
Discussion & Questions
History
General Questions:
- Is this your first pregnancy? Any previous pregnancies?
- Duration of pregnancy?
- When did you find out you were pregnant?
- Any previous antenatal care or visits so far?
- Do you know your blood group? (Important for Rh-negative)
- Any past medical or surgical history?
- Any allergies?
- Any current medications, including methadone or buprenorphine?
- Any concerns about fetal movements yet?
Obstetric History:
- Any past pregnancies, miscarriages, or terminations?
- Mode of delivery?
- Any complications like preterm birth, growth restriction, or stillbirth?
Drug Use History:
- How long have you been using heroin?
- Route of use (smoking, snorting, injecting)?
- Frequency and last use?
- Desire or attempts to stop? Any previous detox or rehab?
- Have you increased your dose recently?
- Time or effort spent on procuring the drug?
- Interference with quality of life or relationships?
- Involvement of violence or coercion?
- Are you on any substitution therapy (methadone, buprenorphine)?
Systemic History:
- Psychiatric: Mood, depression, anxiety (screen for co-existing mental health issues)
- Sexual Health: STIs, contraception use, partner status
- Social: Support at home? Financial situation? Stable housing?
- Smoking/Alcohol/Other drugs?
- Domestic abuse screening
- FGM screening (routine in booking)
Examination
With consent and chaperone:
- General: BP, HR, temperature
- BMI and nutritional status
- Skin signs: needle marks, abscesses, poor dentition
- Venous access assessment
- Urinalysis
- Fundal height (later gestation)
- Doppler for fetal heart (if applicable)
Addressing Concerns (Reassurance & Education)
- “You’ve done the right thing by attending today. We’re here to support you and your baby.”
- “I know this can be difficult to talk about—everything you say is confidential unless there are safety concerns.”
- “We’ll work together with a team to make your pregnancy as healthy as possible.”
Possible Effects of Heroin Use
On the Mother:
- Irregular periods, increased risk of miscarriage, infection, thrombosis
- Malnutrition, infections (HIV, Hepatitis B/C)
- Mental health issues, poor dental health
- Increased risk of DVT, pulmonary embolism, anaemia, and cardiac infection (endocarditis)
On the Baby:
- Premature birth, growth restriction, low birth weight
- Neonatal Abstinence Syndrome (withdrawal symptoms after birth)
- Sudden infant death syndrome (SIDS), neurodevelopmental problems
- NOT linked to congenital anomalies
Management
Antenatal Care:
- Refer to a specialist multidisciplinary team: obstetrician, drug and alcohol services, mental health, safeguarding, social worker
- Urine toxicology at booking (with consent)
- HIV, Hepatitis B & C, syphilis, STI screening
- High-dose folic acid, vitamin D
- Serial growth scans for fetal monitoring
- Dental referral due to increased risk of decay
- Mental health support – IAPT or perinatal mental health services
Opioid Substitution Therapy:
- Continue current stable dose of methadone or buprenorphine (1st line)
- Avoid sudden withdrawal (“cold turkey”)
- Monitor for compliance and illicit use
Intrapartum Care:
- Birth at a consultant-led unit
- Early IV cannula due to poor veins
- Continue opioid therapy in labour
- Avoid naloxone at birth unless essential (can trigger severe withdrawal in baby)
- Continuous fetal monitoring in labour
- Consider paediatric input at delivery
Postnatal Care:
- Observe baby for signs of NAS (Neonatal Abstinence Syndrome)
- Provide more analgesia than routine (opioid tolerance)
- Avoid drugs with high relapse potential (oxycodone)
- Involve safeguarding team if needed
- Support with breastfeeding, contraception, social and financial help
Closure
- Offer written information (PIL) on heroin use and pregnancy
- Arrange MDT follow-up and consultant review
- Discuss contraception postnatally
- Reinforce that care is supportive, not judgmental